

Featured Articles

Praesum Healthcare Services Announces Acquisition by Mayfair Group
Lake Worth, FL – Praesum Healthcare Services today announced its acquisition by Mayfair Group, marking a strategic partnership that strengthens…

Why Does Sharing Experience, Strength and Hope Work?
In order for me to recover, I have to understand at least some of the ideas flitting around in my…
Understanding Dual Diagnosis: Navigating the Intersection of Addiction and Mental Health
Dual diagnosis, also known as co-occurring disorders, presents one of the most complex challenges for individuals struggling with both a substance use…
The Rise of the Sober Curious Movement
As a trend, younger generations have grown more intentional than previous generations in reevaluationg their wellness choices—whether it’s consuming more…

National Recovery Month 2024
PRAESUM HEALTHCARE BEHAVIORAL HEALTH SERVICES IN SIX STATES JOIN IN CELEBRATION OF NATIONAL RECOVERY MONTH 2024 “Recovery is for Everyone:…

Greening Out: The Modern Risks Of Cannabis Use
Greening Out: The Growing Hazards Of Cannabis Use “Greening out” is a new phrase referencing a state of feeling ill…
Children of Alcoholics Week
Praesum Healthcare and Sunrise Detox Spotlight Children of Alcoholics Week Growing up with a parent struggling with substance use disorder…
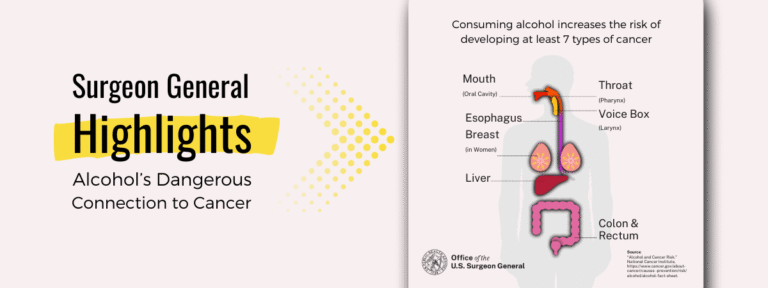
Surgeon General Identifies Serious Alcohol and Cancer Risk
Sunrise Detox Center breaks down the Surgeon General’s warning and what it means for you.
The Rise of the Sober Curious Movement: Rethinking Alcohol in Modern Culture
From the East Coast and beyond, Gen Z has cut down on their drinking. What is this trend Sober curious,…